
OTEZLA XR ONCE-DAILY IS AVAILABLE 1
OTEZLA:
4 INDICATIONSOtezla® (apremilast)/Otezla XR™ (apremilast) is indicated for the treatment of adult patients with plaque psoriasis who are candidates for phototherapy or systemic therapy.Read more

OTEZLA XR ONCE-DAILY IS AVAILABLE 1
*Estimates of patients treated reflect global data since launch (Apr 2014-Mar 2023; US=59% of data). Calculations based on observed drug utilization parameters and number of units distributed. Utilization patterns change over time to best represent current markets.
FDA, U.S. Food and Drug Administration; PsA, psoriatic arthritis; TB, tuberculosis.
References: 1. Otezla [package insert]. Thousand Oaks, CA: Amgen Inc. 2. Data on file, Amgen Inc. 3. Otezla® (apremilast) FDA approval letter. March 21, 2014.

Skin

Scalp
—Genine, an actual patient compensated for her time

Itch
—Genine, an actual patient compensated for her time

Nail

Genital Area
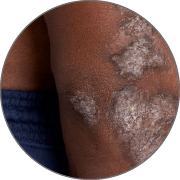
PATIENTS WITH DARKER SKIN TONES ARE MORE LIKELY TO HAVE UNDIAGNOSED PSORIASIS.
Plaques may be thicker, purple in color, and have more scaling. 10
REGARDLESS OF WHERE PLAQUE PsO MANIFESTS, IT IS OFTEN MORE THAN SKIN DEEP FOR PATIENTS 11,12

of patients with mild to moderate plaque psoriasis reported feeling “embarrassed or self-conscious because of their skin” 13,*

of patients with mild to moderate disease perceived their severity to be worse than their affected BSA in the UPLIFT survey 14,†,‡

of psoriasis patients on therapy have cycled through 3 or more topicals and have not used an advanced therapy 15,§
RISK FACTORS OF DEVELOPING PSORIATIC ARTHRITIS INCLUDE:

of patients with psoriasis are at risk of developing psoriatic arthritis 16

higher risk of developing psoriatic arthritis compared to patients without scalp involvement 17,**

higher risk of developing psoriatic arthritis compared to patients without nail involvement 17,**
*According to a US cross-sectional survey conducted among 175 adult systemic-naïve patients with mild to moderate plaque psoriasis (BSA ≤10%). †Based on the UPLIFT survey, a multinational online survey conducted from March 2 to June 3, 2020, including adult patients (≥18 years of age) who reported that they had been diagnosed with plaque psoriasis and/or psoriatic arthritis by a healthcare professional. 1006 patients were surveyed in the United States. ‡In the UPLIFT survey, mild disease was defined as ≤3 palms of affected area and moderate disease was defined as 4-10 palms of affected area. §Data based on active psoriasis patients on therapy between June 2023 to May 2024. Analysis is based on IQVIA Longitudinal Access and Adjudication Dataset (LAAD) claims. IQVIA LAAD is an open claim data source and does not have 100% patient capture. Additionally, the stability rules minimize patient capture changes within the dataset. Advanced therapies included biologic, pre-biologic, and systemic treatments. **In a population-based setting, among 1633 patients first diagnosed with plaque psoriasis, 97 subjects were diagnosed with psoriatic arthritis according to the CASPAR criteria. Cox proportional hazard models were used to identify predictors of psoriatic arthritis within the psoriasis cohort.
BSA, body surface area; CASPAR, Classification of Psoriatic Arthritis; PsO, plaque psoriasis.

Contraindications
Otezla/OTEZLA XR is contraindicated in patients with a known hypersensitivity to apremilast or to any of the excipients in the formulationWarnings and Precautions
Hypersensitivity: Hypersensitivity reactions, including angioedema and anaphylaxis, have been reported during postmarketing surveillance. If signs or symptoms of serious hypersensitivity reactions occur, discontinue Otezla/OTEZLA XR and institute appropriate therapyContraindications
Warnings and Precautions
Adverse Reactions
Use in Specific Populations
Please click here for the full Prescribing Information.
References: 1. National Psoriasis Foundation. Psoriasis statistics. psoriasis.org/psoriasis-statistics/ Accessed March 28, 2025. 2. Pariser D, Schenkel B, Carter C, et al; Psoriasis Patient Interview Study Group. J Dermatolog Treat. 2016;27(1):19-26. 3. Mrowietz U, Kragballe K, Reich K, et al. Arch Dermatol Res. 2011;303(1):1-10. 4. Blakely K, Gooderham M. Psoriasis (Auckl). 2016;6:33-40. 5. Strober BE, van der Walt JM, Armstrong AW, et al. Dermatol Ther (Heidelb). 2019;9(1):5-18. 6. Van de Kerkhof PCM, Reich K, Kavanaugh A, et al. J Eur Acad Dermatol Venereol. 2015;29(10):2002-2010. 7. Kimmel GW, Lebwohl M. Psoriasis: overview and diagnosis. In: Bhutani T, Liao W, Nakamura M, eds. Evidence-based Psoriasis: Diagnosis and Treatment. Springer; 2018:1-6. 8. Pasch MC. Drugs. 2016;76(6):675-705. 9. Merola JF, Qureshi A, Husni ME. Dermatol Ther. 2018;31(3):e12589. 10. Kaufman BP, Alexis AF. Am J Clin Dermatol. 2018;19(3):405-423. 11. Bhutani T, Haberman R, Khattri S, et al. The Psoriasis and Psoriatic Arthritis Pocket Guide. psoriasis.org/the-pocket-guide/. 12. Schafer PH, Parton A, Capone L, et al. Cell Signal. 2014;26(9):2016-2029. 13. Gupta S, Garbarini S, Nazareth T, et al. Dermatol Ther (Heidelb). 2021;11(6):2057‑2075. 14. Lebwohl M, Ogdie A, Merola JF, et al. Presented at: 2021 Maui Derm for Dermatologists; January 25-29, 2020; Maui, HI. 15. Data on file, Amgen; May 2024. 16. Mease PJ, Armstrong AW. Drugs. 2014;74(4):423-441. 17. Wilson FC, Icen M, Crowson CS, et al. Arthritis Rheum. 2009;61(2):233-239.