First and only oral therapy approved for mild, moderate, and severe plaque psoriasis, and active PsA SEE THE DATA
Plaque Psoriasis
OTEZLA:
4 INDICATIONSOtezla® (apremilast)/Otezla XR™ (apremilast) is indicated for the treatment of adult patients with plaque psoriasis who are candidates for phototherapy or systemic therapy.Read more


OTEZLA XR ONCE-DAILY IS AVAILABLE 1
*Estimates of patients treated reflect global data since launch (Apr 2014-Mar 2023; US=59% of data). Calculations based on observed drug utilization parameters and number of units distributed. Utilization patterns change over time to best represent current markets.
FDA, U.S. Food and Drug Administration; PsA, psoriatic arthritis; TB, tuberculosis.
References: 1. Otezla [package insert]. Thousand Oaks, CA: Amgen Inc. 2. Data on file, Amgen Inc. 3. Otezla® (apremilast) FDA approval letter. March 21, 2014.
Hypothetical patient
Paula
Presentation:
Treatment History:
Patient Considerations:
Hypothetical patient

PALACE 1-3 studied DMARD-experienced patients
PALACE 1-3 Study design: Multicenter, randomized, double-blind, placebo-controlled Phase 3 trials. Adult patients with active PsA were randomized 1:1:1 to receive either Otezla 30 mg BID, Otezla 20 mg BID, or a placebo for 24 weeks 1
PALACE 1-3 Primary endpoint: In PALACE 1, Otezla significantly improved ACR20 response vs placebo: 38%, Otezla (n=168) vs 19% placebo (n=168), with or without DMARDs, at week 16; P=0.0001 (nonresponder imputation; FAS). Consistent results were seen with PALACE 2 and 3 1,2
PALACE 4 studied DMARD-naïve patients, like Paula
PALACE 4 Study design: Phase 3 multicenter, randomized, double-blind, placebo-controlled, parallel-group study of 527 DMARD-naïve adult patients with active psoriatic arthritis 3,4
Primary endpoint:

Nearly 2x the ACR20 response rate at 16 weeks with Otezla 30 mg BID (31%, n=176) vs placebo (16%, n=176, P=0.001) 4,*
*Primary endpoint; nonresponder imputation; FAS.
cDAPSA Disease Activity Score 5,6,†


The cDAPSA composite score places patients into one of four disease activity levels 5
cDAPSA Disease Activity Levels


†cDAPSA is calculated as a composite score based on SJC, TJC, PAP, and PtGA with possible scores ranging from 0-154. ‡Clinical remission does not mean drug‑ free remission or complete absence of disease.
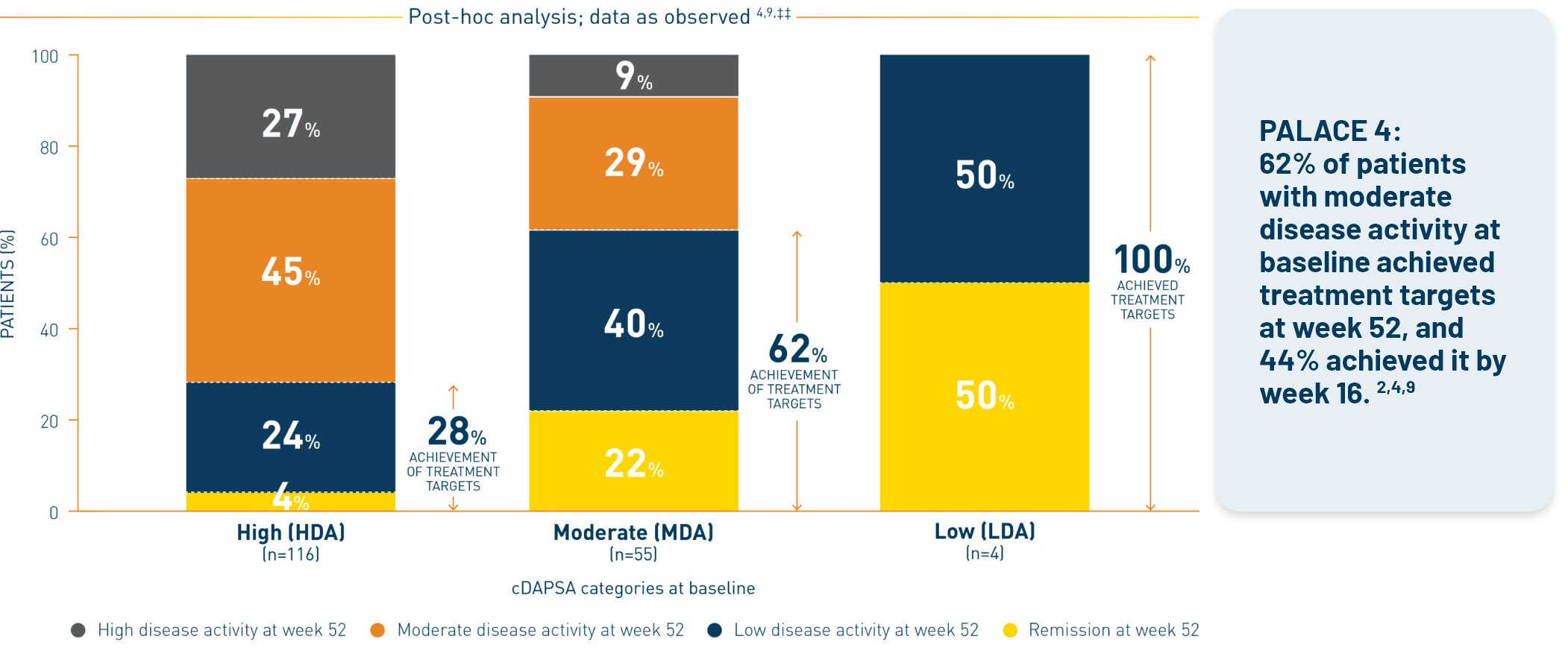
Post-hoc analysis is exploratory and has not been adjusted for multiple comparisons. No conclusions of statistical or clinical significance can be drawn.


PALACE 1-3: DMARD-experienced patients (post-hoc analysis; MI) 5,††
– 37% achieved treatment targets by week 16
§cDAPSA is calculated as a composite score based on SJC, TJC, PAP, and PtGA with possible scores ranging from 0-154. **The post-hoc analyses included patients from the PALACE 1-3 and 4 clinical trials receiving Otezla 30 mg BID who had undergone randomization at baseline and had cDAPSA components available to calculate responses (PALACE 1-3, n=494; PALACE 4, n=175). ††Includes randomized patients who received Otezla 30 mg BID at baseline and had available cDAPSA components at baseline (PALACE 1-3, n=494; PALACE 4, n=175). ‡‡Clinical remission does not mean drug-free remission or complete absence of disease. §§REM or LDA.

In PALACE 1-3
***Not included in the cDAPSA treatment target calculation.
Post-hoc analysis is exploratory and has not been adjusted for multiple comparisons. No conclusions of statistical or clinical significance can be drawn.
ACR, American College of Rheumatology; BID, twice daily; BMI, body mass index; cDAPSA, clinical Disease Activity Index for Psoriatic Arthritis; CRP, C-reactive protein; DMARD, disease-modifying antirheumatic drug; FAS, full analysis set; MASES, Maastricht Ankylosing Spondylitis Enthesitis Score; MI, multiple imputation; NSAID, nonsteroidal anti-inflammatory drug; PAP, Patient Assessment of Pain; PASI, Psoriasis Area and Severity Index; PsA, psoriatic arthritis; PtGA, Patient Global Assessment of Disease Activity; SJC, swollen joint count; TJC, tender joint count; VAS, visual analog scale.

Contraindications
Otezla/OTEZLA XR is contraindicated in patients with a known hypersensitivity to apremilast or to any of the excipients in the formulationWarnings and Precautions
Hypersensitivity: Hypersensitivity reactions, including angioedema and anaphylaxis, have been reported during postmarketing surveillance. If signs or symptoms of serious hypersensitivity reactions occur, discontinue Otezla/OTEZLA XR and institute appropriate therapyContraindications
Warnings and Precautions
Adverse Reactions
Use in Specific Populations
Please click here for the full Prescribing Information.